Triglycerides are important organic compounds. Most of the fat we consume in our diet is triglyceride and so too is most of the fat we store in our body. Fatty acids contained in triglycerides are an essential source of energy for our cells.
Triglyceride concentration can be measured in blood and may provide valuable information about metabolism and general health. High levels may reflect underlying metabolic disorders and evidence shows that high blood triglycerides are associated with increased risk of heart disease (1,2,3).
Just like other types of fats, triglycerides are transported in the bloodstream by lipoproteins. Lipoproteins consist of cholesterol, triglycerides, phospholipids and protein. The lipoproteins act as carriers transporting fats to the organs of the body. Chylomicrons and very low-density lipoprotein (VLDL) are examples of triglyceride-rich lipoproteins.
Recent studies have provided compelling evidence that blood levels of triglyceride-rich lipoproteins are causally related to the development of coronary heart disease (4).
Although high triglycerides may be caused by inherited or inborn lipid disorders, they often result from acquired metabolic abnormalities that can to a large extent be corrected by lifestyle change.
advertisement
Triglyceride-Rich Lipoproteins
High blood levels of triglycerides are most often associated with high levels of the two most important triglyceride-rich lipoproteins; chylomicrons and VLDL.
Chylomicrons are formed in the intestine after a meal. They contain triglycerides and small amounts of cholesterol.
Chylomicrons are subsequently broken down by an enzyme called lipoprotein lipase into free fatty acids that are utilized for energy production by the heart and skeletal muscles or stored in fat (adipose) tissue.
The chylomicron remnants are then removed from the circulation by liver cells.
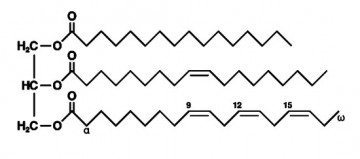
Triglycerides are composed of three molecules of fatty acids attached to a glycerol molecule.
VLDL is produced by liver cells. It transports both triglycerides and cholesterol. Once in the circulation, VLDL is broken down by lipoprotein lipase in capillary beds, releasing triglycerides for energy utilization by cells or storage in adipose tissue.
After triglycerides are released from VLDL, its composition changes and it becomes intermediate-density lipoprotein (IDL). Later, when the amount of cholesterol increases, IDL becomes low-density lipoprotein (LDL).
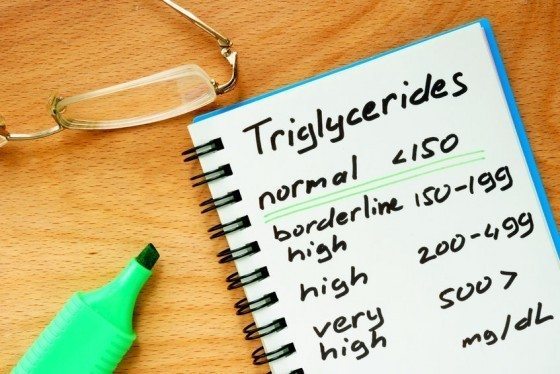
Definition of Normal and High Levels of Triglycerides
Blood levels of triglycerides are stratified according to population data and their associated risk of coronary artery disease. In the USA triglycerides are measured in mg/dL but in Australia, Canada, and most European countries they are measured in mmol/L.
To convert from mg/dL to mmol/L, divide by 88.5
Here is how triglyceride levels are looked at in terms of cardiovascular risk:Normal: <150 mg/dL (1.7 mmol/L)Borderline high: 150 to 199 mg/dL (1.7 to 2.2 mmol/L)High: 200 to 499 mg/dL (2.3 to 5.6 mmol/L)Very high: ≥500 mg/dL (≥5.7 mmol/L)
The term hypertriglyceridemia is used to describe high blood levels of triglycerides.
Hypertriglyceridemia is a relatively common disorder. In the United States, 33 percent of adults have triglyceride levels above 1.7 mg/dL and 18 percent have levels above 2.3 mmol/L (5).
Triglycerides and Cardiovascular Disease
Whether there is a causal association between blood levels of triglycerides and cardiovascular risk is still debated. In other words, it remains uncertain whether high triglycerides cause atherosclerosis. While cholesterol accumulates in atherosclerotic plaques in large quantities, triglyceride accumulation is minor.
Other conditions associated with high triglycerides, such as insulin resistance, a preponderance of small LDL particles, and low HDL cholesterol, may also play an important causative role when it comes to atherosclerosis.
Reduced activity of lipoprotein lipase, which is common in insulin resistance, may slow the clearance of triglyceride-rich lipoproteins from the circulation. VLDL remnants may enter the vessel wall or be converted to small LDL particles. Small LDL particles tend to circulate for a longer duration where they become susceptible to oxidation, glycation, and glyco-oxidation leading to increased risk of atherosclerosis.
Small dense LDL particles appear more strongly associated with the risk of cardiovascular events than larger particles (6,7). In the SCRIP trial, high triglyceride levels were associated small, dense particles in 90 percent of subjects whereas lower triglyceride levels were associated with larger buoyant particles in 90 percent of subjects (8).
Triglyceride-rich remnant lipoproteins can penetrate the arterial wall and may be easily retained. It has been suggested that the atherogenic potential of these lipoproteins is mainly due to their cholesterol content, often called remnant cholesterol (9).
High concentration of triglyceride-rich lipoproteins is associated with low levels of HDL-cholesterol. This is a result of an exchange of lipids between triglyceride-rich lipoproteins and HDL-cholesterol leading to triglyceride-enriched HDL particles low in cholesterol. Low levels of HDL cholesterol are known to be associated with increased risk of heart disease (10).
Apolipoprotein C-III (apo C-III) is found on the surface of triglyceride-rich lipoproteins. High levels of apo-C-III are associated with high triglyceride levels and increased risk of cardiovascular disease. Apo-C-III may contribute to the development of atherosclerosis by several mechanisms. The gene most strongly associated with plasma triglyceride levels is the gene encoding for apo-C-III, called APOC3 (2).
advertisement
Hypertriglyceridemia
The blood concentration of triglycerides is controlled by several metabolic mechanisms involving enzymes such as lipoprotein lipase, cholesteryl ester transfer protein (CETP) and hepatic lipase.
Triglycerides may become elevated with obesity, physical inactivity, high-carbohydrate diet, smoking, diseases such as diabetes and renal failure, drugs such as estrogen, tamoxifen and corticosteroids, and genetic disorders (familial hypertriglyceridemia, familial combined hyperlipidemia, and familial dysbetalipoproteinemia).
There are several types of familial hypertriglyceridemia. These disorders are associated with increased risk of coronary artery disease (11) which appears independent of cholesterol levels (12).
Serum triglyceride values above 1000 mg/dL (11 mmol/L) are rare (less than 1/5000 individuals). The serum in these patients is opalescent due to an increase in VLDL or milky due to elevated chylomicrons.
People with very high triglycerides are at risk of acute pancreatitis (inflammation of the pancreas) which is characterized by abdominal pain, nausea, and vomiting (13).
Hypertriglyceridemia and Cholesterol
High triglycerides reflect an increase in triglyceride-rich lipoproteins such as chylomicrons, VLDL, and IDL. It is important to understand that these lipoproteins also transport cholesterol. Therefore, hypertriglyceridemia is often associated with increased levels of blood cholesterol.
However, chylomicrons and large VLDL particles transport relatively small amounts of cholesterol. Therefore, an elevation of these lipoproteins only produces a mild increase in blood cholesterol. An elevation of cholesterol becomes more pronounced when hypertriglyceridemia is due to an accumulation of small VLDL, beta-VLDL, or IDL particles, as these lipoproteins are often rich in cholesterol.
Management of High Triglycerides
Non-Pharmacological Therapy
Lifestyle modification is the first-line therapy for people with elevated triglycerides.
Many individuals with high triglycerides have insulin resistance and metabolic syndrome (14). In these cases, hypertriglyceridemia is often associated with visceral obesity (15), low levels of HDL cholesterol, high blood pressure and type 2 diabetes. For these patients, weight loss, regular physical exercise, and avoidance of added sugars (16) are all important. Other risk factors such as smoking and high blood pressure should also be addressed (17).
Following a fatty meal, blood levels of triglycerides will rise. However, it is important to understand that raised blood triglycerides following a meal (postprandial hypertriglyceridemia) are caused by chylomicrons produced in the intestine, whereas elevated fasting levels are due to VLDL produced from triglycerides in the liver. The latter is often a result of excessive carbohydrate intake.
Chylomicrons disappear from the circulation soon after the triglycerides have been delivered to the tissues. Thus, moderate fasting hypertriglyceridemia is usually due to increased VLDL.
Fatty acids used by the liver to produce VLDL are derived mainly from two sources. Firstly, during conditions such as obesity, diabetes, and insulin resistance, there is increased fatty acid flux from adipose tissue to the liver. Secondly, there is an increased de novo synthesis of fatty acids in the liver mainly from carbohydrates.
For this reason, in mild to moderate hypertriglyceridemia, losing weight and reducing carbohydrate intake (especially high glycemic index foods and high fructose foods) can lower VLDL and triglycerides.
Dietary fat is not a significant source of liver triglyceride (15), and high fat diets usually don’t raise fasting triglycerides.
The situation may be different in more severe hypertriglyceridemia (above 500 to 1000 mg/dL (5.6 to 11.3 mmol/L)), where the clearance of chylomicrons becomes very slow. Under these circumstances, it is crucial to reduce dietary fat intake to lower triglycerides.
It is necessary for patients with severe hypertriglyceridemia to avoid alcohol abuse as it can cause substantial increases in triglyceride levels and cause acute pancreatitis.
Pharmacological Therapy
Several drugs are used for the management of hypertriglyceridemia.
Although statins are not very effective for lowering triglycerides per se, they are often used to reduce the risk of cardiovascular events in patients with hypertriglyceridemia.
It is still uncertain whether drug therapy targeted at lowering triglycerides will lower cardiovascular risk (16).
One of the most commonly used drug to lower triglycerides is gemfibrozil (17). Gemfibrozil belongs to a group of drugs called fibrates which lower triglycerides by increasing the synthesis of lipoprotein lipase which increases the clearance of triglycerides. Fibrate therapy with either fenofibrate or gemfibrozil can reduce triglyceride levels by 20 to 50 percent. In severe hypertriglyceridemia, gemfibrozil may lower triglycerides as much as 70 percent (18).
In the Helsinki Heart Study, a clinical benefit of gemfibrozil therapy was found in the group with a triglyceride level >201 mg/dL (2.3 mmol/L) and an LDL-C/HDL-C ratio >5.0 (19).
The VA-HIT trial assessed the efficacy of gemfibrozil in patients with low HDL cholesterol, relatively low LDL cholesterol, and mild to moderate hypertriglyceridemia (20). Gemfibrozil raised HDL cholesterol by 6 percent, lowered triglycerides by 31 percent, but had no significant effect on LDL cholesterol. At five years, there was an absolute risk reduction of 4.4 percent with gemfibrozil.
In the ACCORD Lipid trial, fenofibrate improved outcomes in type 2 diabetes in a subset of patients with elevated triglyceride levels and low HDL cholesterol (21).
Nicotinic acid at doses of 1500 to 2000 mg daily can reduce triglyceride levels by 15 to 25 percent (22). However, studies supporting a clinical efficacy of nicotinic acid are lacking. There is data suggesting worsening of glycemic control when nicotinic acid is administered to patients with type 2 diabetes (23).
The AIM-HIGH trial studied the addition of nicotinic acid to statin therapy in patients with atherosclerotic cardiovascular disease and LDL cholesterol levels of less than 70 mg/dL (1.81 mmol/L)(24). There was no incremental clinical benefit from the addition of nicotinic acid during a 36-month follow-up period, despite significant improvements in HDL cholesterol and triglyceride levels.
Intake of fish oil (25) can lower blood triglycerides by as much as 50 percent (26). Relatively high doses of omega-3 fatty acids (EPA + DHA) are needed to achieve this effect (up to 3-4 g/day).
Lovasa (Omecor) and Vascepa are commercial preparations of omega-3 fatty acids that can lower blood triglycerides by as much as 45 percent (27,28).
In patients with refractory hypertriglyceridemia, combinations of statins, fibrates, nicotinic acid, and fish oil are typically used.
No comments:
Post a Comment